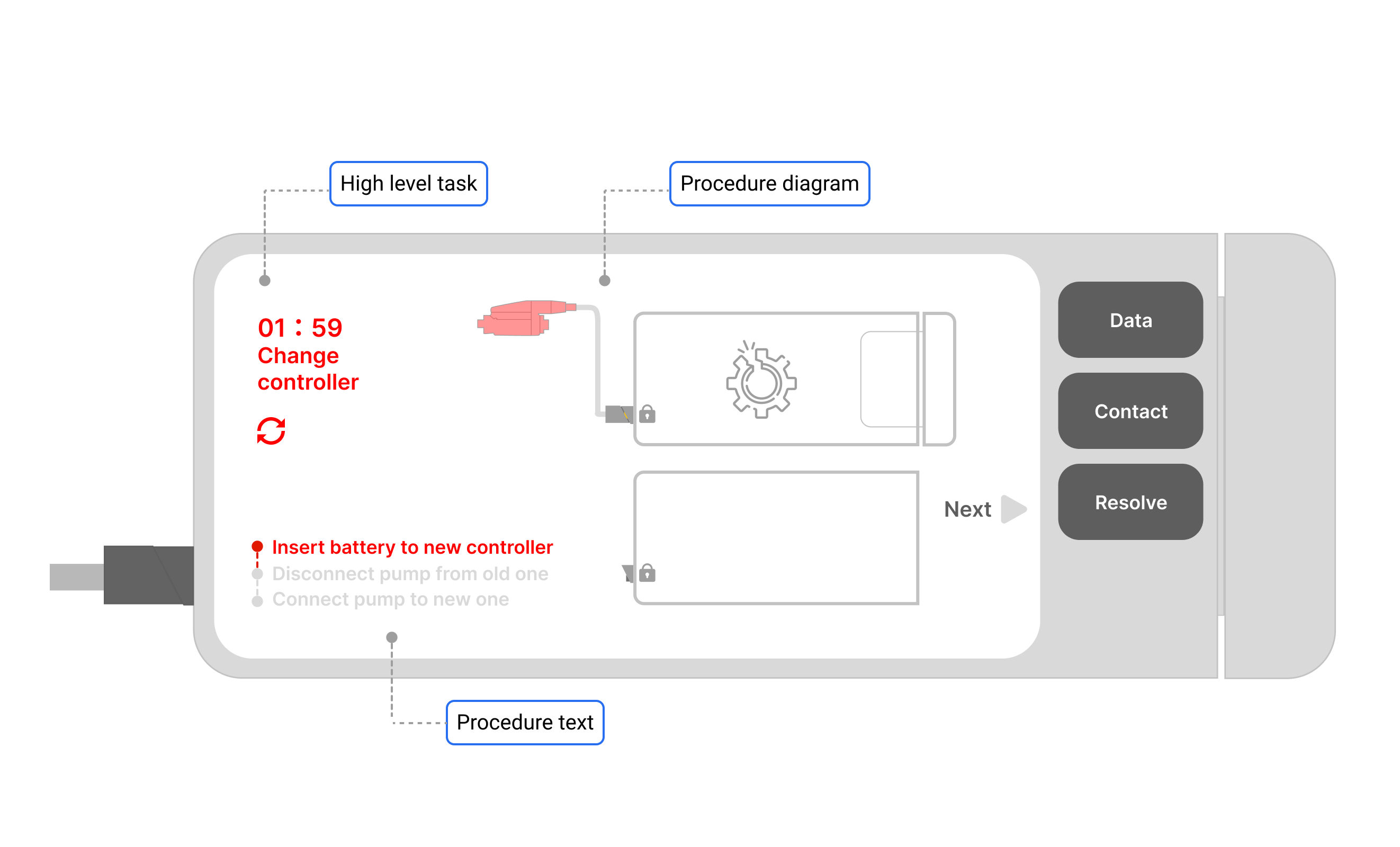
Universal Design is Life-Critical: Unlike commercial products where errors might lead to frustration or minor inconveniences, emergency response interfaces must work flawlessly across all user groups. This project reinforced that true accessibility isn’t merely about language accommodation—it demands universal visual communication through carefully selected icons and imagery that transcend cultural and linguistic barriers. When lives are at stake, there’s no room for misinterpretation.
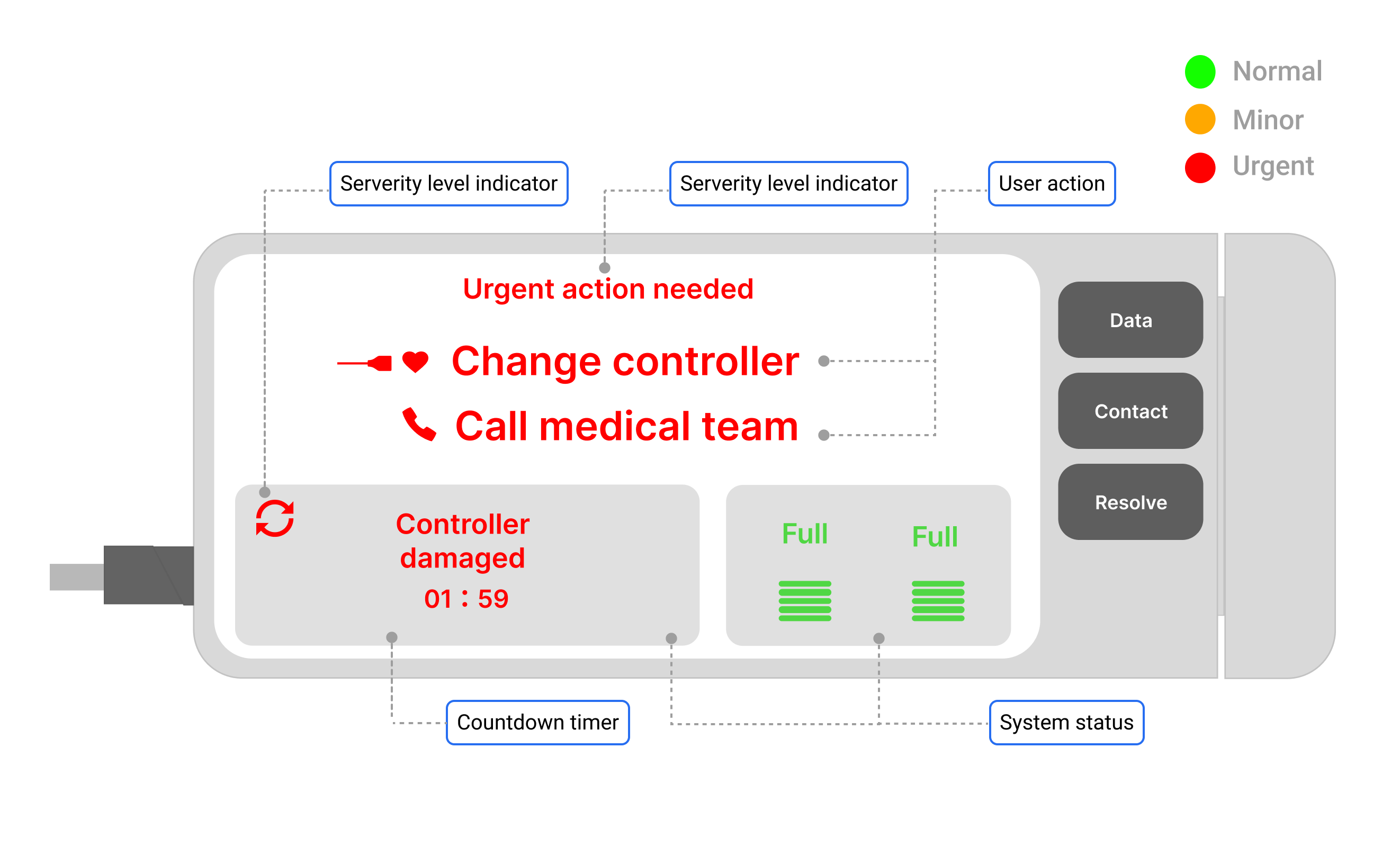
The Urgency-Calm Paradox: One of the most fascinating challenges was striking the delicate balance between conveying appropriate urgency while promoting the calm, focused mindset necessary for effective troubleshooting. This tension represents a unique design challenge that requires thoughtful color psychology, pacing of information, and reassuring interaction patterns that guide users without overwhelming them.
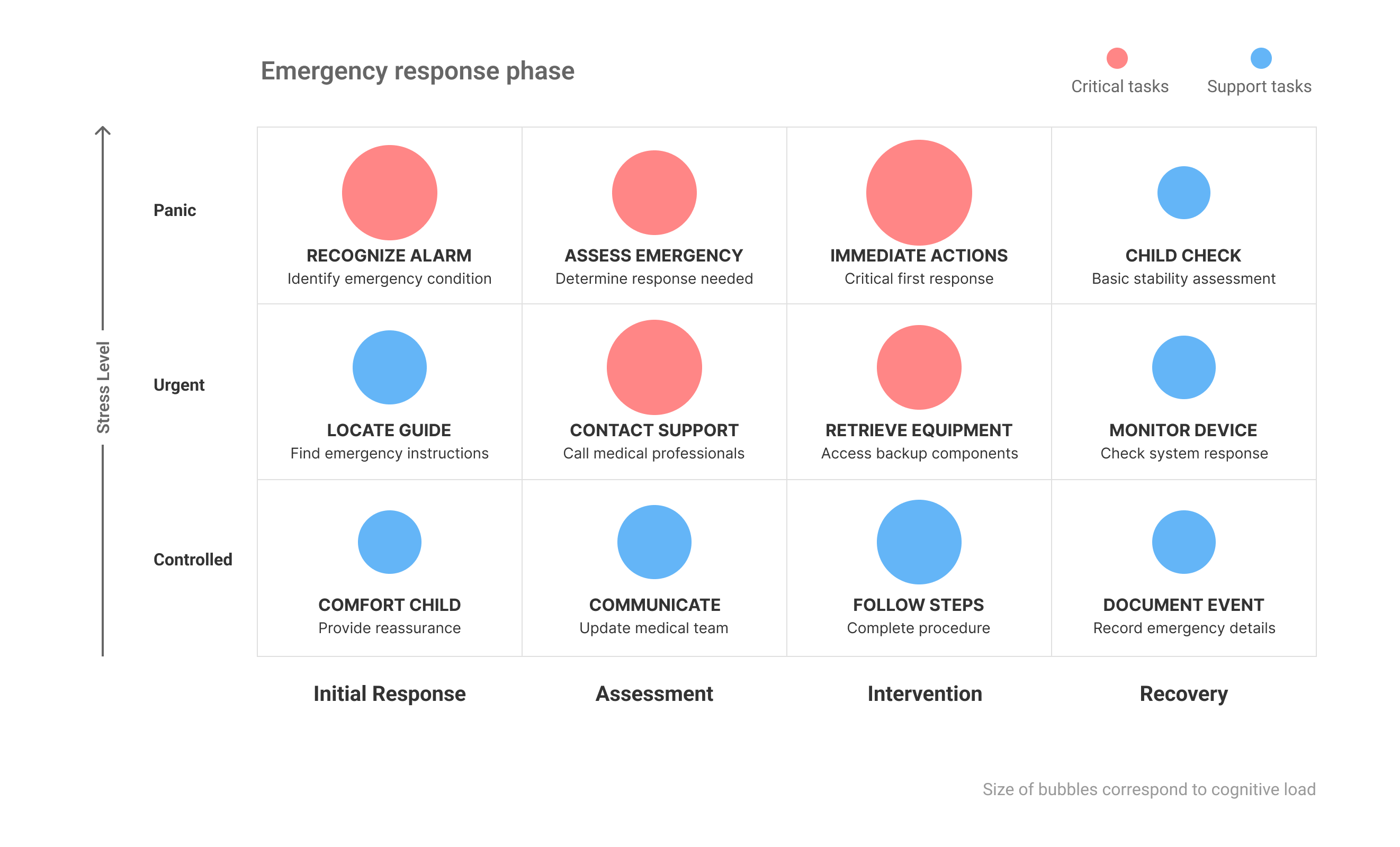
Demographic Considerations: The research revealed how significantly demographic factors influence emergency response behavior. Age, technical literacy, and prior experience with emergency situations all shaped how users interpreted and interacted with the interface. These insights reinforced the importance of designing with diverse user scenarios in mind rather than assuming a one-size-fits-all approach.
Simulation Testing Imperative: If I could revisit this project with additional resources, implementing simulated emergency scenarios would be my top priority. While our controlled testing provided valuable insights, observing users under conditions that more closely mimic the stress and constraints of actual emergencies would yield more authentic data about cognitive processing and decision-making under pressure.